

Abstract

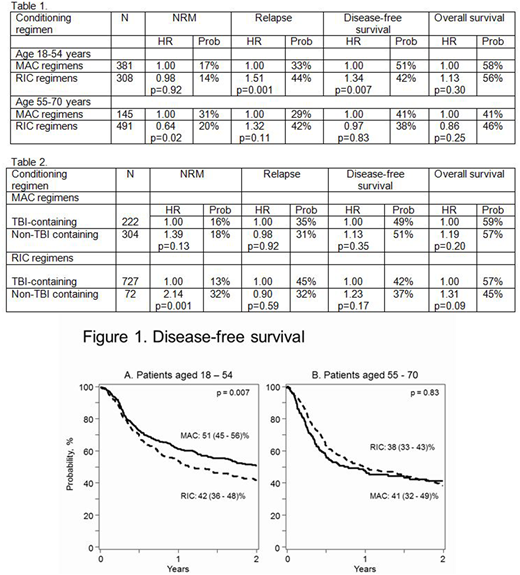
The significance of conditioning regimen intensity on the outcomes of T-cell replete HLA-haploidentical transplants is not known. This study compared outcomes of commonly used myeloablative (MAC) to reduced intensity (RIC) conditioning regimens in 1325 such transplants (AML; n=818; ALL; n=286 and MDS; n=221) in the US between 2008 and 2016. The median age of the study population was 54 years (18 - 70). Most patients (80%) with AML and ALL were in first or subsequent remission; 83% of those with MDS had refractory anemia with excess blasts at transplantation. Fifty-one percent of patients with AML and ALL had intermediate disease risk index (DRI). In contrast, 50% of patients with MDS had high or very high DRI. Patients received MAC (n=526; 40%) or RIC (n=799; 60%) transplant conditioning regimens and a uniform graft-versus-host disease (GVHD) prophylaxis: post-transplant cyclophosphamide, calcineurin inhibitor and mycophenolate. Approximately 50% of patients reported a HCT-CI score of 0-2 in MAC and RIC groups. Sixty-six percent of MAC and 42% of RIC recipients received peripheral blood grafts. Total body irradiation (TBI) + fludarabine (TBI/Flu; 33%) and busulfan with cyclophosphamide with/without Flu (Bu/Cy ± Flu; 36%) were the predominant MAC regimens. Other MAC regimens included TBI/Cy or other agents (10%), Flu/Bu4 (13%), melphalan (140 mg/m2) + Flu ± thiotepa (Flu/Mel ± TT; 9%). TBI (200cGy)/Cy/Flu (84%) was the predominant RIC regimen. Other RIC regimens included TBI 200cGy + Bu or Mel + Flu (7%), Flu/Bu2 (1%) and Flu/Mel (100mg/m2) ± TT (5mg/kg) (8%). The primary endpoint was disease-free survival (relapse or death). Cox regression models were built to study the effect of conditioning regimens on transplant outcomes after adjusting for other factors significantly associated with outcomes. Differences in transplant-outcomes were observed between ages 18-54 years and 55-70 years. The effect of age was further tested within the 18-54 and 55-70 age groups and there were no differences in outcome. In patients aged 18-54 years (n=689), 55% received MAC and 54% received RIC regimens. In patients aged 55-70 years (n=636), 22% received MAC and 78% received RIC regimens. Table 1 shows the effect (hazard ratio; HR) of conditioning regimen intensity in the two age groups adjusted for HCT-CI, recipient CMV serostatus, disease, DRI and graft type and the 2-year probabilities for the outcomes of interest. In patients aged 18-54 years who were equally likely to receive MAC or RIC regimens, relapse risks were higher after RIC regimens that resulted in lower disease-free survival. There were no differences in non-relapse mortality (NRM) or overall survival by conditioning regimen intensity. In patients aged 55-70 years who were more likely to receive RIC regimen, NRM was lower after RIC but without an advantage for relapse, disease-free or overall survival. Figure 1A and 1B show the 2-year probability of disease-free survival by conditioning regimen intensity in patients aged 18-54 and 55-70 years, respectively. Consistent with the main analysis, a subset analysis limited to AML also confirmed higher relapse (HR 1.43, p=0.03) and lower disease-free survival (HR 1.38, p=0.02) after RIC regimens in patients aged 18-54 years but not in patients aged 55-70 years. Acute GVHD (HR 1.01, p=0.94) and chronic GVHD (HR 0.82, p=0.14) did not differ by conditioning regimen intensity. Table 2 compares the effect of TBI- and non-TBI containing MAC and RIC regimens adjusted for age, HCT-CI, recipient CMV serostatus, disease, DRI and graft type. NRM risks were higher after RIC non-TBI compared to RIC TBI regimens. The predominant RIC non-TBI regimen was Flu/Mel (100mg/m2) ± TT (5mg/kg). In conclusion, a MAC regimen offers higher disease-free survival for those aged 18-54 years and can tolerate MAC regimens. For patients who are unable to tolerate MAC regimens, regardless of their age, TBI200 cGy/Cy/Flu is preferred to Flu/Mel ± TT to minimize NRM risks.
Shah:Juno Pharmaceuticals: Honoraria; Lentigen Technology: Research Funding; Exelexis: Equity Ownership; Geron: Equity Ownership; Miltenyi: Other: Travel funding, Research Funding; Oncosec: Equity Ownership. Brunstein:Gamidacell: Research Funding. Champlin:Otsuka: Research Funding; Sanofi: Research Funding. Hamadani:Celgene Corporation: Consultancy; Merck: Research Funding; Janssen: Consultancy; ADC Therapeutics: Research Funding; Sanofi Genzyme: Research Funding, Speakers Bureau; Cellerant: Consultancy; Takeda: Research Funding; Ostuka: Research Funding; MedImmune: Consultancy, Research Funding. McGuirk:Gamida Cell: Research Funding; Kite Pharma: Honoraria, Other: travel accommodations, expenses, speaker ; Fresenius Biotech: Research Funding; Pluristem Ltd: Research Funding; Bellicum Pharmaceuticals: Research Funding; Astellas Pharma: Research Funding; Novartis Pharmaceuticals Corporation: Honoraria, Other: speaker, Research Funding. Vasu:Boehringer Ingelheim Inc: Membership on an entity's Board of Directors or advisory committees. Waller:Pharmacyclics: Other: Travel Expenses, EHA, Research Funding; Cambium Medical Technologies: Consultancy, Equity Ownership; Celldex: Research Funding; Novartis Pharmaceuticals Corporation: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Kalytera: Consultancy.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal